
Cystic Fibrosis
Course and Symptoms of Cystic Fibrosis
|
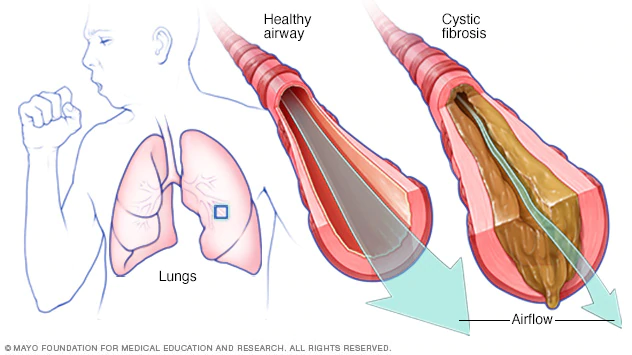
| Image courtesy of MAYO CLINIC Opens in new window Cystic fibrosis (CF) is a chronic and progressive autosomal recessive genetic disease characterized by excessive viscous secretions that interfere with digestion and respiration, resulting in impaired endocrine functioning, with subsequent manifestations affecting the lungs, pancreas, and sweat glands. |
Most clients with CF have exocrine pancreatic insufficiency, and their sweat glands excrete increased sodium and chloride. Even more debilitating is that many of these patients may develop chronic obstructive diffuse pulmonary disease, decreased lung volume, and shunting that result in arterial hypoxemia, possible respiratory failure, and early death.
Prevalence
CF affects people of both sexes and of all races and ethnicities, with the highest prevalence found in Northern European whites. Approximately 30,000 people in the United States have CF, with more than 10 million asymptomatic carriers of the gene for CF.
As with any autosomal recessive disorder Opens in new window, a couple who are both carriers for CF face a 25% risk in each pregnancy of having a child affected with the disorder, a 50% chance of having a child who is an asymptomatic (unaffected) carrier, and a 25% chance of having a child who will neither have nor be a carrier for the disorder.
Symptoms
Symptoms of CF include airway obstruction, chronic infections, pancreatic insufficiency, biliary tract obstruction, and infertility. In 1997, the median survival age for people with CF in the United States was 32.7 years for males and 28.9 years for females.
The symptoms are triggered by a mutation in the gene for a chloride conductance channel, causing abnormally thick and viscid secretions in the respiratory, gastrointestinal, and reproductive tracts.
CF is but one example of a single gene disorder for which one’s ethnicity is a risk factor. Other genetic disorders for which this is true include Tay-Sachs disease Opens in new window and sickle cell disease, which mainly affect different populations and have different symptoms. While many symptoms affect men and women equally, some do not.
In cases of severe CF, pregnancy complications include chronic hypoxia and frequent pulmonary problems. Severe pulmonary infections lead to increased risk for maternal and fetal mortality. Because of the risks involved, female patients with severe CF need information about contraceptive options and, should pregnancy occur, counseling about potential termination as concurrent with the patient’s value system.
Inheritance
To inherit CF, a child must inherit two defective CF genes—one from each parent. Because both partners of a couple are carriers for CF, any child they conceive will be a carrier as well. If both partners are carriers, each pregnancy entails a 50% chance of the fetus having CF. If both partners are carriers, each pregnancy entails a 50% chance of the fetus having CF. If both partners are affected, all of their biological children will have the disease.
Diagnostic Test
The most common test for CF is the pilocarpine sweat test and application of electric current. This test may not be efficacious in newborns, who may undergo an immune reactive test instead. Other tests assess lung and pancreatic function and genetic structure (see Table X1).
| Table X1 | Common Diagnostic Tests for Cystic Fibrosis |
|---|
|
Treatment
Major treatment goals include clearance of secretions, control of infection, and provision of adequate nutrition. Clients with CF must receive preconception counseling. Well-nourished women with mild forms of the disease usually tolerate pregnancy well (McMullen).
See also:
- Dorothy C. Wertz, “The 19-Nation Survey: Genetics and Ethics around the World,” in Dorothy C. Wertz and John C. Fletcher, eds. Ethics and Human Genetics (New York: Springer-Verlag, 1989).
- Dorothy C. Wertz, John C. Fletcher, and John J. Mulvihill, “Medical Geneticists Confront Ethical Dilemmas: Cross-Cultural Comparisons among 18 Nations,” American Journal of Human Genetics 46 (1990): 1200-1213.
- Deborah F. Pencarinha, Nora K. Bell, Janice G. Edwards, and Robert G. Best, “Ethical Issues in Genetic Counseling: A Comparison of M. S. Counselor and Medical Geneticist Perspectives,” Journal of Genetic Counseling 1, 1 (1992): 19-30.
- Institute of Medicine, Assessing Genetic Risks (Washington, DC: National Academy Press, 1994), p. 6.
