
Osteogenesis Imperfecta
Clinical Features of Type IV Osteogenesis Imperfecta
Type IV osteogenesis imperfecta has some similarities to type I but with more severe osseous involvement and less extraskeletal abnormalities. In subtype A, dentinogenesis imperfecta Opens in new window is absent, while it is present in subtype B.
Symptoms of both subtypes include:
- normal sclera,
- normal hearing,
- short stature,
- fractures that begin in infancy (in utero fractures are rare) and
- mild angulation and shortening of long bones.
The genetic defect in types II, III and IV results in a structurally abnormal synthesis of one of the chains of type I collagen.
- General features
Paterson et al have provided the most complete clinical description of this disorder, although Sillence et al first proposed this condition as a separate syndrome.
Segregation in more than two generations and male-to-male transmission have been reported. Evidence thus favors autosomal dominant inheritance. The condition may be less common than type I. Beighton et al have proposed that this disorder is heterogeneous.
Paterson et al determined that, in addition to differences in sclera color compared to osteogenesis imperfecta type I Opens in new window, patients with osteogenesis imperfect IV more commonly have fractures at birth and opalescent teeth.
Bruising and nosebleeds were found to be less common in osteogenesis imperfecta type IV than in type I.
- Facies
Facial appearance is similar to that of osteogenesis imperfecta type I.
- Ophthalmologic abnormalities
Sclera are usually normal, although they may be pale blue in early childhood. Paterson et al noted that no adolescents or adults with the condition had abnormal sclera.
- Otolaryngologic findings
In type IV patients over 30 years old, the frequency of hearing impairment (30%) is significantly less than that in osteogenesis imperfecta type I.
- Neurologic manifestations
Basilar impression resulted in neurologic signs and symptoms in the family with dominant osteogenesis imperfecta, opalescent teeth, and wormian bones reported by Hurwitz and McSwiney; scleral color, however, was not mentioned.
- Cardiovascular system.
A few reports describe a tendency to aortic root dilatation.
- Joint abnormalities
A frequency of joint hypermobility, joint dislocations, and hernias similar to that found in osteogenesis imperfecta type I is noted in type IV.
- Skeletal abnormalities
About 25% of patients have fractures at birth. There is wide variation in the total number of fractures. However, fractures frequency is maximal during childhood but decreases markedly after puberty.
Some individuals with this syndrome may never have fractures. Sillence et al proposed that some patients have a progressively deforming phenotype; thus, it might be difficult in some cases to distinguish this syndrome from osteogenesis imperfecta type III Opens in new window.
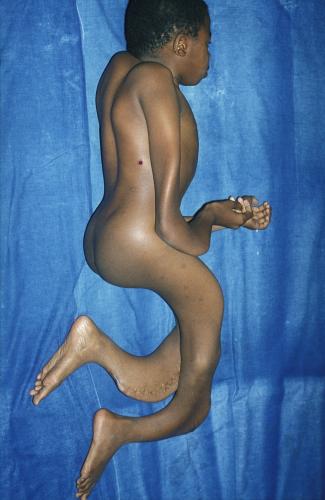 Figure X-1. Photo courtesy of MERCK MANUAL Opens in new window
Figure X-1. Photo courtesy of MERCK MANUAL Opens in new window |
| This photo shows a patient with severe osteogenesis imperfecta who has a barrel chest, spinal curvature, severe bone deformities, loose joints, and poor muscle development. |
Although radiographs taken at the time of first fracture may show no osteoporosis, with repeated fractures, osteoporosis and cystic changes are found.
Stature is generally significantly decreased: 40% of newborns have a length below the tenth centile, and the height of 95% of affected adults is below the third centile. The frequency and average number of wormian bones in the skull in this syndrome are unknown.
- Oral findings
Dental findings are similar to those found in osteogenesis imperfecta type I Opens in new window. Dentinogenesis imperfecta Opens in new window was reported to be either consistently present or consistently absent in a family.
Dental abnormalities are significantly more common in type IV (37%) than in type I (8%). It was also noted that these abnormalities, when present, were the one consistent marker within a family, although other clinical features might vary. Thus, specific dental abnormalities, when present in a family, may be very helpful for diagnosis when other clinical abnormalities are mild.
- Other features
A tendency toward bruising, and excessive sweating has been noted.
See also:
- Clinical Features of Type I Osteogenesis ImperfectaOpens in new window
- Clinical Features of Type II Osteogenesis ImperfectaOpens in new window
- Clinical Features of Type III Osteogenesis ImperfectaOpens in new window
- Osteogenesis Imperfecta (Molecular Pathogenesis of the syndrome)Opens in new window
- Therapeutics for Patients with Osteogenesis ImperfectaOpens in new window
- Sillence DO et al: Genetic heterogeneity in osteogenesis imperfecta. J Med Genet 16:101-116, 1979.
- Beighton P et al: Skeletal complications in osteogenesis imperfecta. A review of 153 South African patients. S Afr Med J 64:565-568, 1983.
- Paterson CR et al: Osteogenesis imperfecta with dominant inheritance and normal sclerae. J Bone Joint Surg Br 65:35-39, 1983.
- Paterson CR et al: Clinical and radiological features of osteogenesis imperfecta type IV. Acta Paediatr Scand 76:548-552, 1987.
- Levin LS et al: Classification of osteogenesis imperfecta by dental characteristics. Lancet 1:332-333, 1978.
- Levin LS et: Scanning electron microscopy of teeth in autosomal dominant osteogenesis imperfecta: Support for genetic heterogeneity. Am J Med Genet 5:189-199, 1980.
