
Personal History
Definition and Importance
Personal history is an account of the personal and social details of a person’s life that includes place of birth, religion, race, marital status, number of children, military status, occupational history, place of residence, education, current living situation, and smoking, alcohol, and drug habits.
The personal and social history is obtained at the initial interview and becomes a part of the permanent record.
The personal history of the individual interviewed is an important component of the pedigree data collection process.
This individual can be the proband—the affected individual who has a specific health history, or the consultand—the individual without a medical problem but whose family history is significant for a disorder.
Therefore, the purpose of conducting a personal history in risk assessment is to identify factors within an individual’s health history that contribute to disease susceptibility, to identify disease characteristics, to facilitate treatment and prognosis of genomic conditions, and to identify environmental risks.
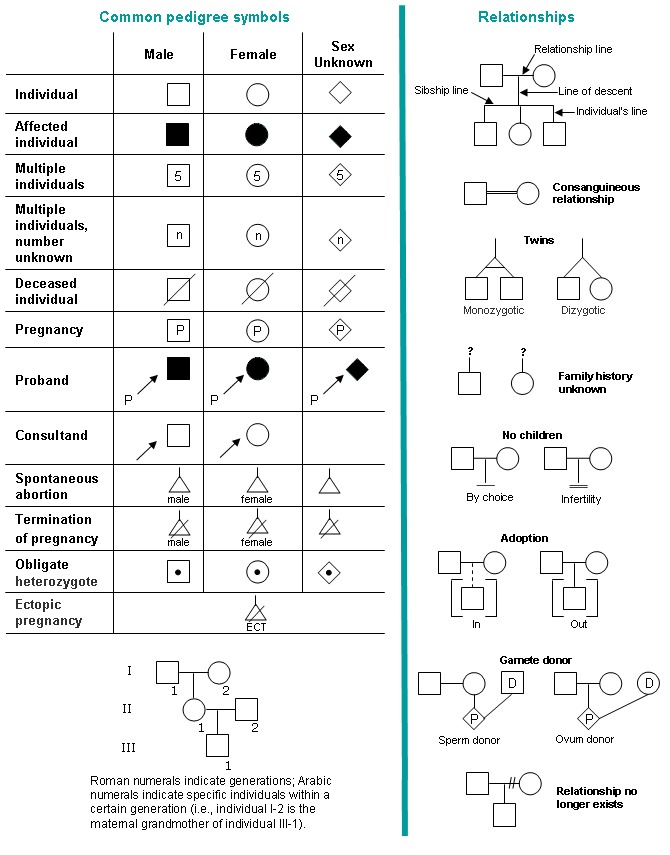
This information is then constructed into a pedigree Opens in new window from the collected family history information, using standardized symbols and terminology. A quick reference is provide in Table X-1.
| Table X-1 | Standardized Pedigree Symbols and Relationship Lines Commonly Used in Family History. |
|---|
|
Personal risk assessment includes a detailed medical, surgical, behavioral, and environmental history; along with information obtained from the physical assessment, and any ancillary, laboratory, and/or pathology data that are important to determining health, disease, and overall disease risk.
The physical examination and/or laboratory and ancillary data may indicate disease risks not apparent in the family history.
Early age of onset of disease or abnormal pathology results might indicate single gene disorders that could be masked by the family history due to adoption, death of family members due to non-genetic causes, or limited family structure.
For example, a female diagnosed with breast cancer at age 40, with tumor characteristics of triple negative disease (hormonal receptors negative for estrogen and progestin and negative for human epidermal growth factor receptor 2 [HER2]) and unknown family history due to her adopted status, represents a personal history of red flags for hereditary breast cancer syndromes, such as hereditary breast and ovarian cancer syndrome (HBOC) due to mutations in BRCA1, BRCA2 and other genes.
This history warrants genetic referral, counseling, and consideration for genetic testing.
Other disorder such as coronary heart disease can be caused by numerous factors, including single gene disorders (e.g., familiarity hypercholesterolemia), or a combination of genomic and environmental factors, including familial or behavioral determinants (e.g., family history of heart disease, obesity, and inactivity).
A thorough personal, family, laboratory, and behavioral assessment may provide the clues to the individual’s disease risk so that strategies can be implemented to reduce that risk.
Personal history encompasses the individual’s medical, surgical, and social history, whereas the family history assessment gives insight into the medical history of blood relatives and, thus, provides a picture of inherited disease susceptibility, as well as complex disorders related to genomic and environmental factors.
For all individuals, basic demographic information in the personal and family history should include the date the history was taken and updated; current age; race/ethnicity; ancestry-of-origin of the maternal and paternal lineage; pertinent medical and surgical data, including psychiatric illnesses and age of onset of the condition; cause(s) of death and age of occurrence; and behavioral history (e.g., tobacco and alcohol use).
Pertinent reproductive history (e.g., history of stillborn, congenital anomalies, spontaneous abortions [miscarriages], pregnancy complications, infertility) should also be part of the assessment.
In addition, data obtained from the history should be depicted in the pedigree Opens in new window, as well as any consanguinity Opens in new window. Stage of life often determines the generalized areas of focus during the data collection process, including physical assessment.
For example, in infants and children, the focus is on proper growth and development. During the teen and young adult years, the focus is on behavioral risks and any known diseases that will influence their transition to adulthood (e.g., sickle cell disease Opens in new window or carrier state), as well as stages of development (e.g., Tanner stage) and reproductive history.
In adults, besides the basic health history information, the personal history may focus more on the reproductive history and gynecologic/obstetrical history.
If the individual (or couple) is of reproductive age and they do not have children, it is important to establish and document if this is by choice or if there is a biological cause for the infertility (e.g., azoospermia, multiple miscarriages, or endometriosis).
During the reproductive years, preconceptual counseling maximizes the chances of a healthy pregnancy, in which, based on the individual and family history, recommended genetic screening tests can be ordered on the parents so that appropriate counseling can take place prior to conception.
Once the child is born, infants and pediatric patients require a detailed birth history that includes any gestational problems or illnesses experienced by the mother, family history of birth defects, and gestational age at birth.
In the geriatric population or older adult, personal and family history includes much of the same data as the adult history but differs because it usually focuses on elderly individuals with complex problems, and the emphasis is on functional disabilities and potential risk for harm (e.g., fall risk).
A complete geriatric assessment may be warranted and performed by multiple personnel (e.g., medical, social work) over many encounters and is best suited for elders with multiple medical problems and significant functional limitations.
An important part of the personal medical history data collection process includes documentation of laboratory values (e.g., complete blood count and indices, cholesterol), pathology and radiographic reports, and a complete review of systems.
- Adapted from: Genomic Essentials for Graduate edited by Diane C. Seibert, Quannetta T. Edwards, Ann H. Maradiegue, Susan T. Tinley
